Sometimes no news is good news. No inflammation, no side effects, no splashy headlines. That’s how it’s been for me this year, finally. Moving into February of 2022, I was able to extend my eye appointments to 6 weeks, 10 weeks, and then 14 weeks apart. The neovascularization quieted down after over a year of regular Avastin injections. Since I had been going in weekly or biweekly for a few months in the winter, dealing with the bleb leak (see Diffusing the Bomb) it was odd(ly refreshing) not to drive to Seattle all the time.
One of the few times I caught myself thinking about my eyes during the summer was at the swimming pool. [Besides the two weeks when I was pretty sick with COVID (even with four vaccinations) and was a little afraid I was going to have to go off my medication (it didn’t happen)].
I swam a decent amount as a kid, and now my kids enjoy lessons. I have two pairs of goggles that fit nicely, but I still hate to wear them. Maybe it’s because my vision isn’t great with them on. Maybe it’s because I’m not swimming laps, I’m up and down and bobbing around, getting splashed by kids, somehow fogging the goggles up.
I’d been avoiding researching just how bad pool water is for folks with eye disease because I didn’t really want to know. I finally did some “googling,” and what I read will give me more motivation to keep my goggles on…
Everyone knows not to go swimming after ocular surgery. I know not to go in after an injection and I didn’t go near the pool during my bleb leak.
In swimming pools, chlorine is used to reduce water-borne bacteria and viruses to prevent pathogens and diseases from spreading. Chlorine is a fairly decent sanitizer, but it doesn’t kill everything. Efficacy is also dependent on how much chlorine is added and how often.
Another thing that chlorine is good at is washing away your tear film. Tear film is made up of three layers and protects your eyes, among other things. Read Facts About Tears.
“When your eyes are submerged in chlorinated pool water, the tear film that usually acts as a defensive shield for your cornea is washed away. This means that your eyes are no longer protected from dirt or bacteria that are not entirely eliminated by the treated pool water. So, swimmers can be prone to eye infections“ (Dr. David WIlliams, OD, https://2020eyecareoh.com/does-chlorine-hurt-your-eyes/)
Conditions such as conjunctivitis are not fun in and of themselves but can cause serious complications for someone with uveitis. Anterior uveitis can be exacerbated by irritation from chlorine or even brought on by parasites, which would be more common in lakes or other water bodies (Water Related Ocular Diseases, Saudi J Ophthalmol., 2018)
Before swearing off swimming altogether, there are things you can do to reduce the impacts of chlorine and avoid infection.
Wear Goggles: Just when you thought the worst part of swimming was swimsuit shopping… finding the right pair of goggles can take a while, but they are the most impactful in terms of protecting your eyes. Goggles can cause a slight increase in interocular pressure, so if you’re in the danger zone (i.e. taking drops or medication to reduce pressure), you probably want to discuss this one with your doctor.
Rinse off after swimming: Make sure that if you don’t have time to shower thoroughly, you at least use clean water to rinse off your eyes and face.
Use Drops: Preservative-free drops are very helpful when combating dry eye and rinsing out anything that is causing irritation to the eye. Additionally, you could even talk to your doctor about using a drop like Ofloxacin (prescription antibacterial) sparingly if you swim a lot and are worried.
One thing about posterior uveitis is that without microscope and imaging technology, diagnosing and managing the disease would be nearly impossible. It’s never lost on me (or my insurance bill) how these advanced cameras let the outside world in on what is going on in the back of my eyes.
When I see a machine like this one, I see beauty in the technology that is allowing my doctor and me to preserve my vision:
optos.com
A brief definition of tools, tests, and terminology can be found here.
This post is a summary of the imaging I get done every 4-6 weeks when my eyes are active.
Fundus photography
A fundus camera is basically a microscope with a camera attached which photographs the back, interior part of the eye when the eye is dilated.
“Fundus photography documents the retina, the neurosensory tissue in our eyes which translates the optical images we see into the electrical impulses our brain understands. The retina can be photographed directly as the pupil is used as both an entrance and exit for the fundus camera’s illuminating and imaging light rays,” according to the overview excerpted from Saine and Tyler’s Ophthalmic Photography, as posted on the Ophthalmic Photographer’s Society’s website. The page contains a detailed description of the process.
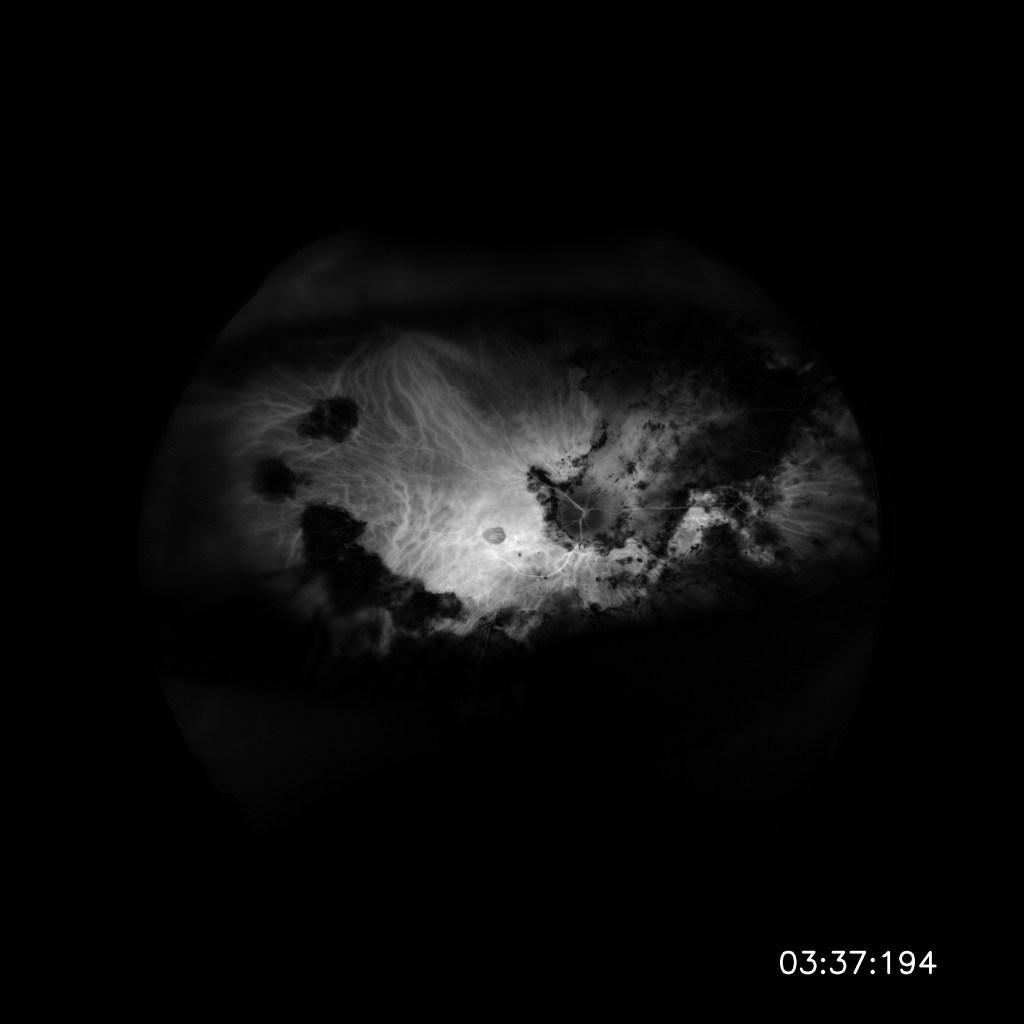
Top Image: Normal Eye (Retina Image Bank) the bright spot is the location of the optic nerve ***** Bottom Image: My right eye with tons of lesions and scaring from past inflammation due to uveitis. These are the areas that I cannot see through when they are in my field of vision. (8/28/2020)
Fundus photography is a valuable technology. Photographs can be used for comparisons from visit to visit and year to year which enables doctors to notice even minute differences inside the eye that may not be noticeable by simply looking at current conditions. Photographs also leave less room for details lost to memory, interpretation and error in note-taking. Although there is, of course, still room for artifacts of the images, shadows, or simply that angle and magnification are not always easy to replicate.
Angiography
Fundus photography of the vessels in the retina can be done with different filters or with specialized dyes, which is called angiography (“to write or record vessels”). Angiography is used to diagnose conditions such as choroidal neovascularization. The dye is injected into an arm vein of the patient and then retinal photographs are taken.
Intravenous fluorescein angiography (IVFA) uses a dye called sodium fluorescein which fluoresces in yellow-green and produces high contrast in the vessels so to see enlarged or leaky vessels in the retina. Indocyanine green (ICG) is another type of dye but fluoresces in the infrared range which makes it easier to see vessels even when there is fluid or hemorrhaging around the area. It is used to highlight the choroid. Both dyes are highly concentrated and will take about a day to pass through your system (i.e. expect neon urine). Angiography is not recommended while pregnant.
IVFA of my right eye on 8/28/2020
ICGA of my right eye on 8/28/2020
Optical Coherence Tomography
Optical Coherence Tomography (OCT) uses light waves to document a cross-section of the tissue layers of the retina. This test enables your doctor to map and measure the thickness of the layers and note any irregularities. Like fundus photography, OCT is non-invasive, and in my opinion, is much easier on the eyes due to the lack of flash and the fact that you can blink at any time during the exam.
I’m fortunate to go to the Karalis Johnson Retina Center at the University of Washington Eye Institute, which is not only a clinic but a research facility with the latest technology. The Retina Center recently opened in a new location with new imaging equipment and the difference is night and day in terms of eye fatigue from having photos taken. The flash is so much less bright. This makes it easier to keep eyes open to take the photos. Technicians are looking for photos at angles and magnifications comparable to those previously taken.
OCT of my right eye. Notice the bump of fluid from the vessel (that’s not supposed to be there) due to choroidal neovascularization. (08/28/2020)
Want to learn more?
The Optos Virtual Showroom is kind of a fun, interactive website if you want a look at what a $200,000 camera looks like and the kinds of photographs it produces!
I’ve spent this year going to the University of Washington Medical’s Karalis Johnson Retina Center on a monthly basis in an attempt to get my uveitis under control. Last winter, in addition to prednisone, I started taking Cellcept, first 1000mg twice a day, then 1500mg twice a day.
Cellcept (mycophenolate) is an anti metabolite, which slows down the immune system, and is most often used as an anti-rejection medication after organ transplants. (Read about uveitis treatments here). It gave me an upset stomach at first, but a month in, I no longer experienced that side effect. The worst part about Cellcept for me is just the timing of taking it. You can’t eat an hour before or two hours after taking it, which means I have to get up and take it awhile before breakfast and I have to schedule my Saturday night snacking around it. This I can handle.
Yet Cellcept, in addition to 20 mg of prednisone was still not controlling my inflammation. So, we introduced Humira, which is a self-administered injection to the thigh or stomach every other week. Humira is a “biologic” that blocks a protein called TNF-alpha, which is believed to be produced in excess in those with non-infectious uveitis.
I can’t say I’ve noticed any side effects specifically from the Humira. In my experience, the company goes almost overboard with assistance. The only thing I don’t like is that it is mailed in a large styrofoam box every month (with ice packs to keep it cold), which I feel guilty about throwing away. I even tried to give the boxes away online… Surprisingly no one wants medication boxes during a pandemic… go figure.
Cellcept and Humira are both known to take a few months to reach full efficacy, so I received two Ozurdex injections in the spring.
In terms of overall side effects, I have noticed I am bruising super easily, am more dried out than before and my hair is thinning a bit. These are potential side effects of pretty much all immunosuppressants so it’s hard to isolate what’s causing what, or if it’s just the fact that I’m on three different medications. I’m down to 7.5 mg of prednisone at this point, so I’m sleeping much better.
Thus, the good news is, my inflammation seems to be under control. However, in July my optical coherence topography (OCT; see Tools, Tests, and Terminology) showed a bit of fluid in the retina, and there was a new hemorrhage that showed up on my fundus photos. So, I received an Avastin injection.
In August, my doctor had a few diagnostics run. A Fluorescein Angiogram (FA) and Indocyanine Green Angiogram (ICGA), along with another OCT, pointed to choroidal neovascularization membrane (CNVM) or choroidal neovascularization (CNV). This is another side effect of uveitis; it’s listed in the “Terminology” section of my website. [Side note: this experience is making me think that maybe I need to take the “terms” on that page which are actually complications of uveitis and make a separate page that goes further into detail about each. So, stay tuned for that if you’re interested.]
For now, neovascularization means ‘new blood vessels’. When damaged by disease, the retina may produce too much vascular endothelial growth factor (VEGF) which leads to the production of new blood vessels. The blood vessels grow from the choroid into the retina. However, unlike normal vessels, these vessels are leaky and allow fluid from blood or blood cells to enter the retina because the tissue is damaged. (Choroidal neovascular membrane, 2017)
“This fluid can immediately distort the vision because it forms a blister in the retina, which is normally flat. Over the course of days to months, this fluid can damage the retina, killing the light-sensing cells, called photoreceptors” (What is Choroidal Neovascularization?, 2020).
According to one article, CNV is commonly associated with Multifocal Choroiditis, which is what I have, and is found in 32-46% of patients (Neri, Piergiorgi, et al., 2009). Just when I feel like I’ve about filled up my punch card of uveitis complications, I discover I have another!
In September, the swelling looked like it was dying down after the first Avastin injection, so I made the choice not to receive another injection. At my October appointment, however, the fluid and hemorrhage were not gone, so I received the first of my series of three, to be done 4-6 weeks apart.
Speaking of injections, a common side effect of injections or surgical procedures involving the eye is Ptosis, or drooping of the upper eyelid. I had this pretty noticeably after my Retisert implant surgery, so much so that I considered surgery to fix it! Luckily my lid “bounced back.” Lately, since I’ve been seeing myself on all these Zoom and Teams virtual meetings, I feel that my right eyelid is getting there again (my husband says I notice it more than others… which may be the case, but it still bugs me!). I recently read that there is a new drop out to fix this issue. Upneeq was approved by the FDA this year to treat acquired Ptosis (First Prescription Fix for Droopy Eyelid, 2020). I am anxious to try these drops but am choosing to wait until my CNV is resolved before adding in another variable. In the meantime, I’ll continue to just use my eyelash curler in an attempt to keep my right eye looking peppy…
Lastly, because I’ve been on varying dosages of prednisone for quite a while, I had a Dual-energy X-ray Absorptiometry (DEXA) Scan done in 2018. A DEXA scan measures bone mineral density and bone loss, which is a side effect of long term systemic cortical steroid use. At that time, my results showed minor osteopenia in my lumbar spine and left hip. (Read Prednisone: The Good, the Bad & the Ugly Part I and Part II.)
Osteopenia is the precursor to osteoporosis, which is when bones are weak and brittle due to too much bone loss. Since that time, although I have continued to be on steroids, more so this last year than the previous, I have increased my weight-bearing exercise and been very diligent about taking calcium supplements daily.
I had a follow-up DEXA Scan in October and both areas of osteopenia are now in the “normal/ expected range for age.” My bone mineral density increased 3% in the lumbar spine and 1.5% in the left hip. Diet and exercise do work!
So, that’s what’s been going on with my uveitis as of late. Here’s to hoping the new year will bring fewer visits to the Retina Center!
It’s a new season in this crazy pandemic year. With fires blazing, school in session, and elections and holidays on the horizon, life is not easy right now, and on medication, it can be even more challenging to navigate. With that said, the following is Part II of information on Prednisone that I think is useful. Drop me a line if you think I missed something important!
Interactions
In Part I, I discussed interactions with prednisone by way of calcium and potassium absorption (i.e. it inhibits absorption, so supplements are recommended), and also the interactions between insulin and sugar (i.e. limit sugar on prednisone, this includes alcohol). Other interactions include some anti-infectives, anti-diabetic agents, and non-steroid anti-inflammatory drugs (NSAIDs). If you are taking other medications along with prednisone, talk to your doctor, and check interactions on drugs.com or another trusted website (https://www.drugs.com/tips/prednisone-patient-tips).
Tapering and Withdrawal
I’ve tapered down in dosage many times and gone completely off of prednisone a couple of times. The importance of tapering cannot be overstated. In Part I, I talked about Adrenocortical Insufficiency. When on prednisone for more than three weeks, the body becomes reliant on it for cortisol and stops making its own (How do you to taper off prednisone?). So, it’s important to wean your body off the supplemented steroid so it does not crash and leave you with a whole host of painful (and potentially dangerous) withdrawal symptoms. Even with tapering, you may have withdrawal symptoms; the longer you’ve been on prednisone, the more likely it is that you will have them.
Withdrawal Symptoms may include:
Severe fatigue
Joint pain
Fever
Stiff or tender muscles
Body aches
Lightheaded feeling
No appetite
Labored breathing
Vomiting
Weight loss
Headaches
Adrenal crisis, a rare, possibly fatal reaction to a lack of steroid hormone in your body
Depression
Anxiety
For me, fatigue, or just being able to sleep better, is always the first and most common symptom of tapering off of higher doses, All of the bad side effects slowly start to fade away. However, when I have gone to taper off of prednisone, from only 10 mg, even when I thought I was tapering slowly, I have had excruciating joint pain. I was convinced that I had arthritis or another autoimmune condition had been revealed last time I tapered. I would wake up and barely be able to move my fingers! My knees and back just ached. I felt like I was 80 years old! I thought I was insane; I was only coming off of 10 mg! Then I read the following statement, from Adrenal Insufficiency United’s “Glucocorticoid tapering and adrenal suppression testing guide,” which was such a relief to me:
“[Withdrawl] Symptoms are milder at high cortisol amounts and intensify when milligrams are reduced below a certain point. A longer adjustment period is recommended at lower doses.”
The guide linked above includes tapering recommendations. There are others available online, such as these on RheumInfo.com. I recommend reviewing some and thinking about what might work for you; different methodologies exist (stair steps, alternating dosage days, etc) and it might take trial and error to discover to which your body responds best. Take examples to your doctor before you start your taper or if you are experiencing painful withdrawal symptoms. Tapering can take weeks or months, depending on your dosage and the duration of treatment.
Pregnancy and Breastfeeding
I’ve made it no secret that I took a low dosage (~10 mg if I recall correctly) during my two pregnancies and while breastfeeding, and my sons incurred no known side effects. I’m not advocating one way or another, this is just my experience and it coincides with the latest information out there, which is that taking prednisone during pregnancy does not significantly increase the background chance of having a baby born with a birth defect (Mother To Baby, 2018, linked below). I did make the choice to not donate breast milk to anyone because of my medication. I discuss my pregnancy experience in my blog post: Women and Uveitis: my pregnancy journey and I’ll link the articles I cite in the post regarding prednisone here:
I also recommend reviewing Prednisone on “LACTMED” the Drugs and Lactation Database. This page includes information like drug levels detected after certain amounts of time which can be useful in trying to time feedings or pumpings to have the least amount of drug present possible.
COVID-19
Although COVID-19 is a new pandemic, there has already been work done compiling information regarding the impacts for patients on corticosteroid treatment, as well as recommendations for further treatment. I have a handful of links and papers on the home page of this website. Taking immunosuppressants during a pandemic is something to consider carefully.
A collection of COVID-19 cases among 600 patients with rheumatic diseases found that “glucocorticoid use at a prednisone-equivalent dose ≥10mg/day was associated with an increased odds of hospitalisation, which is in agreement with prior studies showing an increased risk of infection with higher dose of glucocorticoids. The study also demonstrated “that most individuals with rheumatological diseases or on immunosuppressive therapies recover from COVID-19, which should provide some reassurance to patients” (Gianfrancesco M, Hyrich KL, Al-Adely S, 2020).
In another paper, 139 uveitis experts from around the globe were given statements and answered questions about treatment options for Non-Infectious Uveitis (NIU) patients and Immunomodulatory Treatment (IMT). [IMT is the treatment of disease by activating or suppressing the immune system. In the case of treating uveitis, the medications are reducing or suppressing the immune system.] Statements were developed around when to initiate, continue, decrease and stop systemic and local corticosteroids, conventional immunosuppressive agents, and biologics in patients with NIU in increased risk, high risk, and very high-risk categories.
This paper contains helpful tables and flow charts on recommendations based on your risk category and specific treatment types.
Summarized results related to corticosteroids:
Surveyed uveitis experts recommended to not begin systemic corticosteroid or immunosuppression for NIU treatment in sick patients with suspected or confirmed COVID-19, irrespective of risk group.
Among sick patients receiving high-dose corticosteroid, consensus was to taper the dose in all risk groups and to taper even low-dose corticosteroid in high-risk patients or very high-risk patients. Tapering instead of abrupt cessation of the oral corticosteroids was recommended in view of the risk of adrenal insufficiency. This paper is full of useful tables and flow charts to follow based on which risk level you’re at.
In healthy patients, experts agreed to start oral corticosteroids only in increased risk patients and not in high-risk or very high-risk patients.
Low-dose oral corticosteroids and conventional IMT should be maintained, while only in increased risk or high-risk patients, higher-dose corticosteroids should not be tapered and stopped.
In healthy patients with a contact history, the overall agreement is lower. Low oral dose corticosteroids and conventional IMT should be maintained in increased risk patients.
Although first-line treatment for NIU consists of local or systemic corticosteroids, overall consensus emerged that in the setting of the COVID-19 pandemic, the use of systemic corticosteroids should be avoided in sick patients and local therapy (regional corticosteroid injections) should be preferred to systemic treatment in all patients, irrespective of their risk and health, except in healthy patients not already on corticosteroids. Systemic corticosteroids might be harmful, given their mechanism of action that inhibits the immune responses and affects the pathogen clearance.
Prednisone was synthesized in the mid-1950s by Arthur Nobile and has since been a miracle and a misery for people with autoimmune and inflammatory disease.
When I first started taking prednisone in 2011, I had no idea what I was in for and it showed. I gained about 10 pounds pretty quickly, “moon face” and all. When my brother came to visit he told me he barely recognized me. I had terrible acne that covered my chest and neck. My knees ached so badly I couldn’t stay in bed, and since I couldn’t sleep anyway, I was up early and late. I was completely miserable.
I was on 40-60 milligrams (mg) at the time, which is a lot. A dose above 40 mg is considered a “high dose,” while anything below 7.5 mg is considered a “low dose” and to be “steroid sparing” (most patients don’t experience the side effects known to be associated with prednisone at this level) (https://www.aocd.org/page/SteroidsOral).
The prednisone did its job; my uveitis was brought to a screeching halt. But I couldn’t stay on the high dosage forever (thankfully) due to all of the side effects. I transitioned to combinations of prednisone and methotrexate and cyclosporine, eventually turning to RETISERT (see Treatments page).
I’ve been on and off prednisone since then, more time on than off, but at a much lower dosage. Typically I’ve been on 5-10 mg with pulses when I have a flare. And, I can honestly say, it’s often the only thing that keeps my uveitis at bay. That’s why prednisone is prescribed so regularly for a myriad of different conditions; it works and it works fast. Although the side effects of prednisone at high doses are likely unavoidable, I now am aware of them, long and short term, and what I can do to lessen them.
Let’s start at the beginning.
What is prednisone and what does it do?
Prednisone is a synthetic glucosteroid. It is a type of corticosteroid that is closely related to and mimics cortisol, which is a hormone naturally produced by the adrenal gland in the body.
When the body becomes stressed, the pituitary gland at the base of the brain releases ACTH (adrenocorticotropic hormone), which stimulates the adrenal glands to produce cortisol.
The extra cortisol allows the body to cope with stressful situations, such as infection, trauma, surgery, or emotional problems. When the stressful situation ends, adrenal hormone production returns to normal.
The adrenal glands usually produce about 20 mg of cortisol per day, mostly in the morning, but they can produce five times that much when needed in a stressful (or perceived to be stressful) situation. Prednisone, the most commonly prescribed synthetic corticosteroid, is four to five times as potent as cortisol. Therefore, roughly 5 mg of prednisone is equivalent to the body’s daily output of cortisol. There are other synthetic corticosteroids available which differ in potency and half-life (Eustice, 2020).
During a stressful scenario your body is in “fight or flight” mode and thinks of little other than dealing with the stressor. Therefore, when you have increased corticosteroids in the body, your body blocks substances that create inflammatory actions called prostaglandins (which initiate healing and deal with allergic reactions) and white blood cells (which destroy foreign cells and allow the immune system to function properly). In this way, corticosteroids suppress the immune system.
Cortisol also helps to control the salt and water balance in the body as well as regulates carbohydrate, fat, and protein metabolism. When you have a heightened amount of corticosteroid in your body, this system too is thrown out of whack. And thus, we have side effects.
Side Effects of prednisone
There are known side effects of prednisone, particularly with prolonged use, for virtually every system in the body. I’ve summarized some of the more common side effects below. Check out Drugs.com for a more complete list and more details.
When reading through some of these, it’s clear that many are connected and all are impacted by daily actions such as diet, exercise, stress response and sleep.
Adrenocortical Insufficiency
When given in a stronger dose than the amount the body can produce on its own, for prolonged periods, glucocorticoids may cause decreased secretion of endogenous (self-made) corticosteroids by suppressing pituitary release of corticotropin (secondary adrenocortical insufficiency). Basically, since you’re taking prednisone, the body senses the level of steroid is “high enough” and stops making as much. This is why it is dangerous to stop taking prednisone cold turkey (I’ll post about tapering off prednisone next month). The degree and duration of adrenocortical insufficiency is highly variable among patients and depends on the dose, frequency and time of administration, and duration of therapy. Talk to your doctor about adrenal supplements and lifestyle changes if you are feeling sluggish and tired all of the time (especially on high doses of prednisone).
Immunosuppression and Increased Susceptibility to Infection
Increased susceptibility to infections is common on prednisone. It’s easier to get sick when the immune system is suppressed. This can mean anything from serious and potentially fatal infections like chicken pox and measles to persistent athlete’s foot and candida. Read Study Warns about higher infection Risk.
Remember that administration of live virus vaccines, including smallpox, is contraindicated (advised against) in patients receiving an immunosuppressive dosage of glucocorticoids. Glucocorticoids, especially in large doses, increase susceptibility to and mask symptoms of infection.
Infections with any pathogen, including viral, bacterial,or fungal infections in any organ system, may be associated with glucocorticoids. There are a variety of ways to get rid of or lessen the severity of infections such as fungal infections, both with and without medication. In my experience, diligence is paramount if you are going to be on prednisone for a while.
Musculoskeletal Effects
Muscle wasting, muscle pain or weakness, and atrophy of the protein matrix of the bone resulting in osteoporosis or osteopenia can all be side effects of prednisone. Osteoporosis and related fractures are one of the most serious adverse effects of long-term glucocorticoid therapy. The American College of Rheumatology (ACR) currently considers patients receiving or planning to receive greater than 2.5 mg of prednisone daily for three months or longer to be at risk for bone loss (Glucocorticoid-Induced Osteoporosis).
A high protein diet may help to prevent adverse effects associated with protein catabolism. Calcium and vitamin D supplementation and weight-bearing exercise that maintains muscle mass are suitable first-line therapies aimed at reducing the risk of adverse bone effects.
I had a Dexascan in 2018 which showed slight osteopenia in my hips. It surprised me because I’ve always been pretty active and wasn’t on a high dose of prednisone at the time (I was nursing my second son at the time which may have contributed). I’ve since increased my calcium and vitamin D and my weight lifting. My insurance covers another scan this December, so we will see if it worked!
I also remember when I was on 60 mg, the pain in my lower back and knees was so bad I would wake up at night and not be able to sleep.
Ocular Effects
As many of us with uveitis know, the treatments often involve the side effect of cataracts and increased intraocular pressure. Prolonged use of prednisone may result in posterior subcapsular and nuclear cataracts and/or increased intraocular pressure (IOP) which may result in glaucoma or may damage the optic nerve if left unchecked.
Nervous System Effects
Side effects of prednisone include insomnia, mood swings, and depression. I tend more toward the “intense” side of personalities at times (hey, I’m a Scoprio.. what can I say?!) and when I’m on higher doses of prednisone I have to consciously remind myself to tone it down a little. Especially when I haven’t slept much due to high doses; I usually notice trouble sleeping when I’m on 20 mg or more. Another side effect I’ve noticed, but don’t generally read in the literature is feeling warm all of the time, which can also impact mood and sleeping. Altering your sleep schedule (can you fit in a nap?) based on when you sleep best can help as well as just giving yourself down time and plenty of grace… and space.. from other people (sort of kidding).
Endocrine and Metabolic Effects
Prednisone may decrease glucose tolerance, produce hyperglycemia (high levels of sugar in the blood), and aggravate or precipitate diabetes mellitus, especially in predisposed patients. If glucocorticoid therapy is required in patients with diabetes mellitus, it may be necessary to change insulin or oral antidiabetic agent dosage or diet. Read What is the link between prednisone and diabetes?
The increased requirement for insulin, accompanied by potassium loss, sodium (and fluid) retention and increased appetite often lead to weight gain when uncontrolled. Monitoring carbohydrate and refined sugar, and sodium intake can help with these side effects. See the Prednisone Friendly Diet from Stop Sarcoidosis and Prednisone Weight Gain by Dr. Megan, Prednisone Pharmacist, who has really great info on her site.
Patients with hypothyroidism may have an exaggerated response to glucocorticoids. Glucocorticoids can lower serum TSH levels and decrease TSH secretion through direct effects on TRH in the hypothalamus. Chronic use of high dose glucocorticoids do not appear to cause clinically significant central hypothyroidism (Haugen, 2009).
Sodium retention with resultant swelling, potassium loss, and elevation of blood pressure may occur, but is less common with prednisone. Along with swelling is the less-than-fun phenomenon known as “moon face.” Read Embrace Moon Face and supplement potassium.
Dermatologic Effects
I’ve always struggled with acne, but let me tell you that prednisone acne is real. When I was on 60 mg, I literally bought turtle necks and wore them all the time because my neck and chest were so broken out (luckily it was winter). Prednisone impairs wound healing (remember, it’s telling your immune system to chill out) which can make acne last longer.
Jack reached out to me through livingwithuveitis.com; it’s been really great to meet folks who are out there reading! He’s been dealing with uveitis for two years and is a web designer on a mission to inform other developers about uveitis.
About you:
Name and age:
Jack Pritchard, 25
Hobbies:
Cycling, software development
Last book you read:
12 Rules For Life, an Antidote to Chaos
3 things you can’t live without during #stayathome:
My plants, Comfort food, Calls with Family and friends
About your uveitis:
What type of uveitis do you have / what is your diagnosis?
Chronic Panuveitis in both eyes
Is your uveitis associated with another condition or disease?
Sarcoidosis
How did you know something was wrong? When were you diagnosed and how long did it take?
I had several incidents following up to the official diagnosis. At first it was flashes of lights in the corner of my eyes, associated with weight lifting. Next I lost vision in my eyes for a week when on holiday. Then finally I arrived in eye casualty in October 2018 to be given an official diagnosis and multiple treatments.
How are you currently treating your uveitis? What other treatments and/or procedures have you tried?
I’ve been on just about any eye drop you can associate with the condition. Maxidex, Iopidine, Monopost, Azarga, to name a few. I’ve also taken a number of pills, including – Prednisone, Methotrexate, and Acetazolamide. At the moment, I’m currently on Mycophenolate and Prednisone. I’ve had several injections to the eye to help with the ‘sticking’ on my pupil which haven’t been effective.
Most recently, I’ve undergone double eye surgery in my right eye. One surgery for cataracts to replace the lens in the back of my eye, and another at the same time to implant a Xen implant or ‘shunt’ to reduce the pressure. I’m currently in discussions to get my left eye done. The surgery has saved my life, and restored peace in my mind, as prior to surgery I was in the most difficult flare up of my life.
What is the hardest part of having uveitis for you?
Being able to function as a normal human, my day job requires me to be able to read screens. Going out with friends in time of flare-ups creates discomfort when in light environments and I’ve altered my home setup to accommodate for my sensitivity to light.
How has having uveitis changed your life?
I cannot begin to describe the ways in which is has altered my life. In times of a flare up, or issues it can cause my life to fall into pieces. On the other hand it has changed my direction in life, which could be seen as a positive.
Do you research uveitis (causes, treatments, etc) or get all your info from your doctor?
A mixture of both. Doctors are great at answering quick fire questions I have on my mind or written down. However, sometimes doctors can easily end up getting highly technical in their speech and that’s when I turn to online resources where others have put it in simpler terms for me to understand or reference.
Do you think people know about uveitis? What do you wish people knew about uveitis?
Very few people know of Uveitis, I don’t expect everyone to know. I wish people knew how difficult it was for us to read text, and how much pain light can cause. As it’s an internal health problem, it’s an invisible condition to those you see on the street. As someone who is 25 years old, nobody makes the assumption that I am suffering from an autoimmune disease which makes it hard to see. Most people can afford sympathy to older individuals as it’s assumed they may have health problems, but younger individuals are assumed to be in good health.
Anything else to add?
I’m currently on a journey to make the world wide web a little bit more accessible to those with Uveitis. As a website developer, I am responsible for developing accessible web pages, and with the introduction of new technologies I have been thinking of different ways I can help, even if small.
To help get a better understanding on how I can help, or what I should build, I am speaking with others that have Uveitis or visually impairing conditions. If you too suffer with any condition, please do get in touch so I can chat with you about your condition and alterations you’ve made to your lifestyle.
We’ve all been staying home for a few weeks now and likely have heaviness in our hearts, so I thought I’d write about a less serious topic. [If you feel like you want to read about COVID-19 as it relates to eye health, head to the homepage where I’ve added a section with coronavirus-related links.]
A question I’ve seen come up in online groups is: “should I wear eye makeup if I have uveitis?” Frivolous and unimportant to some, but a valid question for many of us!
First off, can makeup cause uveitis? No. Uveitis is not an infection and is not caused or exacerbated by wearing eye makeup. Some forms of uveitis are caused by systemic infections or diseases, but that’s a different topic, discussed here.
If you have dry or sensitive eyes, wearing eye makeup may worsen that condition, particularly depending on the makeup ingredients (Impact of Makeup on Dry Eye Disease).
If you’re wearing expired makeup, using dirty brushes or applicators, or sharing makeup, there is a risk of infection or conjunctivitis. This is not fun in itself, (who has toddlers with pink eye?! just me?) but when you have uveitis, it can complicate matters.
Should you get an infection, it is advisable to throw all of your eye makeup away and start fresh. If you wash your brushes exceptionally well, keep them. When in doubt, toss them too. This is inconvenient and expensive (or an excuse to go shopping…). Sometimes infections are inevitable, but the best way to avoid them is to keep your makeup and tools clean and Do. Not. Share.
I’ve always loved wearing makeup and being diagnosed with uveitis hasn’t changed that. It has, however, changed a few of my makeup-related behaviors.
“No makeup” times
Let’s start with when I don’t wear eye makeup. 1) I don’t wear eye makeup to my ophthalmology appointments. 2) I don’t wear makeup after eye surgery until my eyes have healed and I’ve had follow-up appointments. 3) I don’t wear eye makeup after injections until my course of associated antibiotic drops is complete. If I have a hemorrhage, I typically wait until that has cleared before I start wearing eye makeup again. If I had anterior uveitis, I probably wouldn’t wear eye makeup when I was having a flare.
Keep it clean
When I wear eye makeup, I wear clean (as in, non-toxic) makeup. I used to just purchase what was trendy and in cute packaging. Now I research extensively before buying any of my cosmetics. Glitter is out since being diagnosed with uveitis. I don’t buy anything with parabens or phthalates (endocrine disruptors). I check for triethanolamine (TEA) and diethanolamine (DEA) in mascara and eyeliner. TEA and DEA are ethanolamines that break down into nitrogen, which can form nitrosamines. Nitrosamines are carcinogenic (may cause cancer), according to the Environmental Working Group (EWG)’s Safecosmetics.org.
Another ingredient that I personally avoid, but is very pervasive, is talc in eye shadow. According to the EWG, some talc contains carcinogenic asbestos, although it’s required by law to be asbestos-free. Unless you can verify the talc is asbestos-free, it should be avoided. Talc is also an irritant of the eyes for many people (Is talc in makeup safe?).
Ilia Beauty – The Necessary Palettes (Talc Free)
These are my current favorite clean makeup brands:
Ilia Beauty – The Necessary Eye Shadow Palettes, Clean Line Gel Liner, Limitless Lash Mascara,
Jane Iredale – Pure Pressed Eye Shadow, Eye Pencil, PureLash Mascara
Mineral Fusion – Eyeshadow Trios, Eye Pencil, (didn’t love the mascara)
Thrive Causemetics – Infinity Waterproof Liner, Liquid Lash Extensions Mascara, (eye shadow contains talc as the second ingredient)
Tarte Cosmetics – Lashpaint Mascara, (eye shadow contains talc as the second ingredient)
I previously mentioned not using expired makeup. Throw out mascara every 3 months (I attempt to sync mine with changing seasons so it’s easy to remember). Toss eyeliner once a year and eye shadow at least every two years. (When to Throw Away Your Makeup, According to a Dermatologist). If it looks bad, smells bad or you can’t remember when you bought it, it’s probably time to say goodbye.